

What are the most common types of scars you treat at UnionDerm, and how do you determine which treatment approach is best for each patient?
The most common scars we encounter are surgical scars, post-acne scars, traumatic scars, and burn scars. Some scars can become hypertrophic or form keloid scars. During the consultation, the patient’s skin will be examined and analyzed for patient-specific factors like scar age, morphology, pigmentation risk, and if they cause symptoms like itching or pain. Based on goals for treatment outcome, downtime, and timeline for improvement, an individualized scar revision treatment plan will be determined that may include medical, cosmetic, or even surgical treatments for each type of scar.
Can you walk us through the latest technologies you use for scar treatment? How have these advanced compared to older methods, and what results can New York patients expect?
Our office offers combinable and customizable targeted treatments for diverse skin types that can improve the color, texture, and overall cosmetic appearance of scarred skin. We have several techniques for collagen stimulation of thin atrophic scars, intralesional antimetabolites to calm excess collagen production in hypertrophic scars, vascular laser therapy for redness, topical agents and lasers for dyspigmentation, and surgical techniques such as subcision for tethered scars or revision surgery when necessary.
Some laser scar treatment techniques have advanced over the years. For example, compared to older fully ablative laser skin resurfacing methods (CO2), which required weeks or even months for recovery, the modern fractionated technologies stimulate collagen remodeling with significantly less downtime of several days. Newer devices are also combinable, allowing for multi-modal treatment of scars at varying depths of skin, which can accelerate the results (i.e., radiofrequency microneedling or subcision followed by non-ablative fractional resurfacing on the same day).
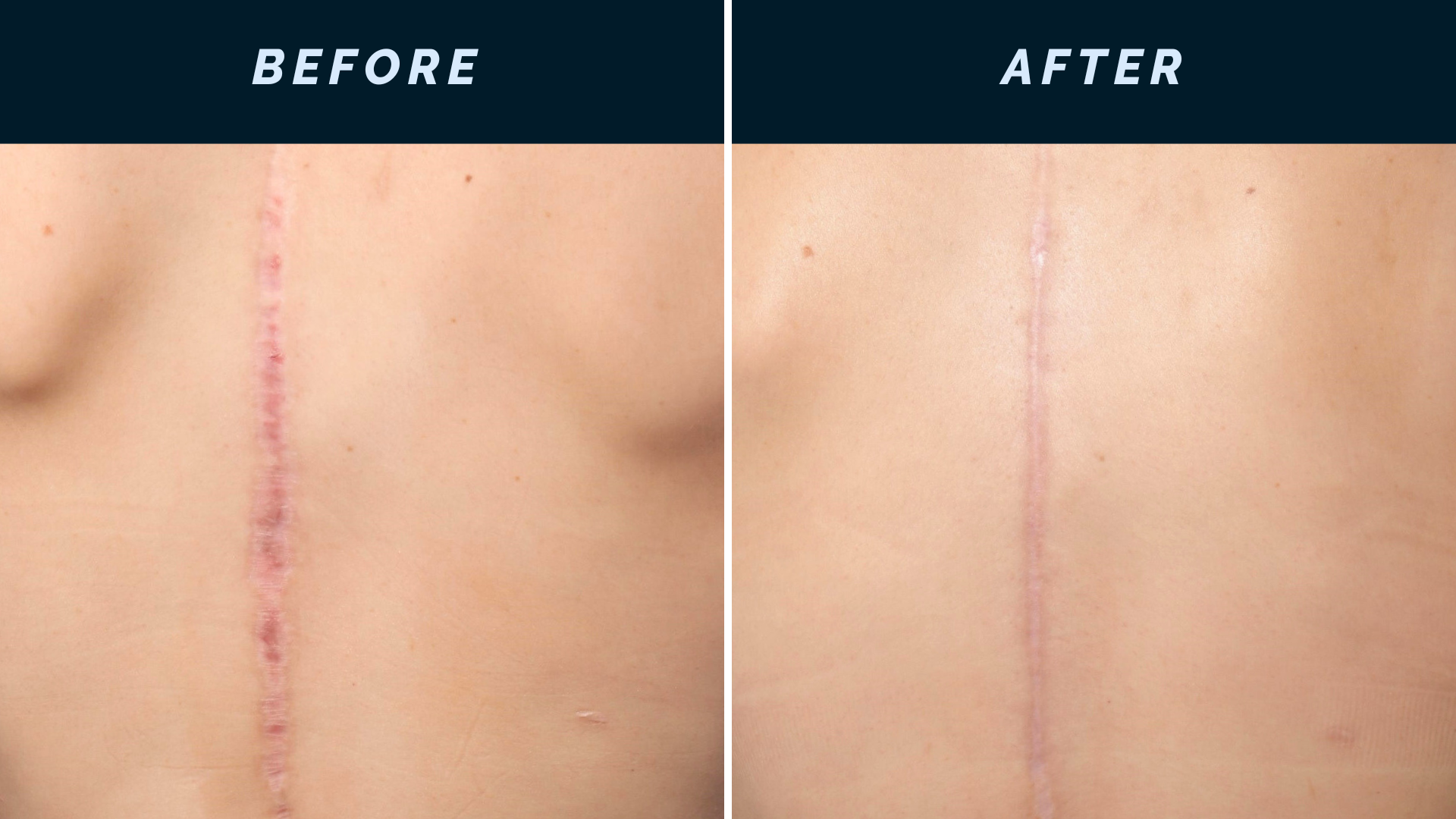
Although most scars are permanent and generally cannot be erased completely, patients can expect gradual improvement in the texture, color, and depth of scars. The goal of treatment is for the skin to appear overall smoother with softened scar edges and a more even tone. After the last treatment, improvement in scar appearance may continue with further collagen remodeling lasting up to a year.
For patients with acne scarring, which is quite common in our New York patient population, what treatment options do you typically recommend and why?
Acne scars are one of the most common skin conditions we treat. But each scar, even on the same person, can have varied morphologies and usually requires a combination approach for optimal results. Examples of acne scar treatments include fractional laser resurfacing (ablative and non-ablative), vascular lasers, radiofrequency microneedling, subcision, high-dose chemical peels (TCA CROSS), biostimulatory fillers, or steroid injections for hypertrophic scars. Depressed scars, such as rolling or boxcar acne scars, often benefit from subcision combined with biostimulatory fillers or fractional laser resurfacing.
When do you recommend surgical scar revision over non-invasive treatments? What factors help you make that determination?
Surgical scar treatments are recommended when a scar is very wide, poorly aligned at the edges, or has significant tension or contracture, where non-invasive approaches alone may not correct the irregularities to the same extent. Scar excision involves removing the scar tissue and re-approximating the surrounding tissue with more favorable tension vectors and better alignment to create a thinner, less conspicuous scar line. Furthermore, laser therapy or injectables can be started early after scar revision to improve the final cosmetic outcome.
How soon after an injury or surgery should someone seek scar treatment, and does early intervention make a significant difference in outcomes?
Intervention is best immediately after surgery or trauma. The initial approach is to optimize the healing process for minimal scarring. Laser treatment, injectables, and conservative home therapy, such as massage or silicone products, can commence as early as 2 weeks after the inciting event and may continue for several months. Since collagen remodeling is a slow process, surgical revision is usually reserved until at least a year after initial scar formation.
What combination treatments have you found most effective for stubborn or older scars? How do you customize treatment plans for different skin types and tones?
Stubborn or severe scars frequently benefit from combination therapy. Some examples of a multimodal approach that can be done on the same treatment day include subcision + fractional laser resurfacing, ablative laser + platelet-rich plasma, biostimulatory fillers + laser resurfacing or vascular lasers, and steroid injections + fractional ablative lasers for laser-assisted drug delivery.
The patient’s skin tone is very important in choosing the best device options to minimize the risk of side effects such as hyperpigmentation. In skin of color, treatments like radiofrequency microneedling and non-ablative laser resurfacing are often safer options than ablative lasers. Customization based on skin type is critical for optimizing results while maintaining safety parameters.
Can you explain the difference between ablative and non-ablative laser treatments for scars? What are the benefits and recovery considerations for each?
Ablative and non-ablative lasers are similar in that they heat water molecules at varying depths of skin, causing microthermal zones of trauma. The controlled injury stimulates the body’s own wound healing response that removes the damaged skin and stimulates intense collagen and elastin production, resulting in smoother scars and tighter, healthier skin.
The main difference between the techniques is that the energy of ablative lasers is high enough to vaporize columns from the surface of the skin to heat deeper layers in the dermis, while non-ablative lasers are gentler and only heat the columns of skin without fully removing the top layers. Ablative lasers are therefore more aggressive, making them better suited to treat raised scars or deeper scars, but with significant downtime that results in weeping, crusting, and swelling that can last 7 to 10 days and residual redness that can linger for 1 to 2 months. Non-ablative treatments have a less intense healing period with no oozing and minimal swelling and dryness during 3 to 6 days of recovery time; however, multiple treatments are required to achieve similar results as one ablative treatment.
What are some common misconceptions patients have about scar treatment, and what would you want them to know about modern scar management options?
One misconception is that surgical procedures can be done with no scars or that the scar will eventually disappear. That is why it is very important for patients to consult with their physician and discuss the risks of scarring prior to any cosmetic or medical procedure that requires cutting or puncturing the skin. Any incision that reaches the depth of the dermal layer will heal by bridging the skin with collagen, which results in the appearance of a scar, and therefore, no surgery can be completely “scarless.” However, a trained and skilled surgeon can design and execute the procedure to minimize scar formation and provide follow-up care for optimal wound healing and scar remodeling post-procedure.
A common misconception is that scars can be completely removed. It is not possible with any of today’s technology to make skin within a scar exactly like healthy skin prior to injury. With the understanding that scars are permanent, modern treatments to treat scars aim to improve texture, reduce visibility, and help the scar blend naturally with the surrounding skin. Patients should also be mindful that sun exposure can darken scar tissue and slow progress, so consistent sun protection is an important part of any scar management plan.
Another misconception is that one treatment can fix everything. Most scars require a series of treatments, a combination of approaches, and time for adequate skin remodeling to achieve perceptible improvement. Fortunately, there are more scientific advances coming on the market, and we have new treatment options that weren’t available even a decade ago.
For patients considering scar treatment, what should they expect during the consultation process at UnionDerm, and how do you set realistic expectations for results?
During the consultation, a detailed scar assessment includes evaluation of scar type, depth, skin pigmentation risk, previous treatments, as well as patient goals, tolerance of downtime, and timeline for improvement. We can then develop a customized treatment plan that usually requires a combination of modalities and several treatment sessions over a period of months to years, since collagen remodeling is a slow biological process and can differ from person to person. The overall goal is a meaningful cosmetic improvement while maintaining natural skin texture and tone.
Are there any new or emerging scar treatment technologies you’re excited about bringing to UnionDerm, and how might these benefit patients who haven’t had success with traditional methods?
An exciting new technology available at UnionDerm is the non-ablative Miria laser by Avava. The unique feature of this laser is the ability to deliver energy through the surface of the skin in a conical array that concentrates the beam at controlled depths in the deeper dermal layers. The advantage is that at the surface, it causes similar improvement and downtime to traditional non-ablative lasers, but deeper layers receive energy close to ablative lasers, achieving collagen remodeling results faster without the weeping, crusting, and downtime of ablative lasers.
One of the most beneficial features, especially in the diverse population of NYC, is that Miria is safe across all skin types, including patients at higher risk of post-inflammatory hyperpigmentation. For patients who haven’t responded well to traditional non-ablative fractional lasers or microneedling, Miria offers more significant collagen remodeling at greater depths, less downtime, and a better safety profile than traditional ablative lasers, with progressive improvement over several months as collagen builds after a treatment series. In practice, we often incorporate Miria into a combination approach, such as pairing with subcision or biostimulatory fillers, for one of the most advanced tools we currently have for non-surgical scar remodeling.